93% of physicians say prior authorization delays patient care. 89% say it fuels burnout. And 37% of PA transactions are still done by fax. In 2026, CMS is forcing the fix — with FHIR APIs, AI auto-approval, and the first-ever PA mandate for Original Medicare.
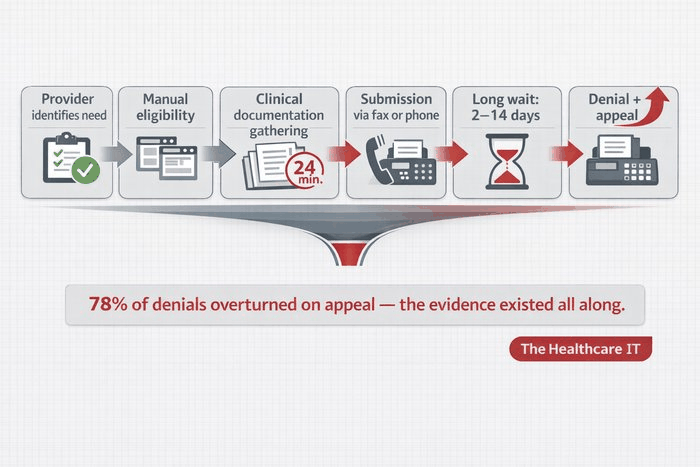
The numbers are staggering: the US healthcare industry spends $14.6 billion annually on prior authorization, a utilization management process where 78% of denials are ultimately overturned on appeal. That means the clinical evidence existed all along — the submission process simply failed to capture it. For CIOs, CTOs, and VPs of Digital Health at Healthcare ISVs, IT services firms, and mid-size clinics, 2026 is the year when PA automation transitions from optional investment to compliance imperative.
What Is Prior Authorization and Why Is It Broken?
Prior authorization is the process by which healthcare providers must obtain pre-approval from a patient’s health insurer before delivering specific medical services, procedures, or prescriptions. The payer reviews whether the proposed care is medically necessary and covered before agreeing to pay. PA applies across commercial insurance, Medicare Advantage, Medicaid managed care, and — as of January 2026 via the WISeR pilot — select services in Original Medicare.
The current workflow is a nine-step chain that breaks at predictable points. Providers identify a need, verify eligibility across multiple payer portals, manually gather clinical documentation (averaging 17–24 minutes per request per the CAQH Index), submit via fax, phone, portal, or X12 278 EDI, wait 2–14 days for a decision, and then fight denials through appeals. According to the AMA’s 2024 survey, physicians complete an average of 39 PAs per week, spending 13 hours on the process. 40% of practices have hired dedicated PA staff. 29% of physicians have seen PA cause serious adverse events including hospitalization.
The economics are equally broken. Manual PA transactions cost providers $10.97 each versus $5.79 for fully electronic transactions (CAQH 2023 Index). Only 35% of medical PA transactions are fully electronic. The remaining 65% flow through fax, phone, and payer-specific web portals — each with different forms, requirements, and interfaces. This fragmentation is the root cause of the $14.6 billion annual administrative burden.
5 Challenges Draining Revenue and Burning Out Your Staff
Multi-portal chaos: A practice with 10 payer contracts navigates 10 different portals with unique submission requirements. There is no single standard submission interface in the current state.
Documentation gaps causing denials: 78% of PA denials are overturned on appeal (Surescripts). The clinical justification existed in the EHR but was not captured in the submission. This is a workflow failure, not a clinical failure.
Decision delays blocking care: Only 12% of clinicians and 7% of administrators consistently received PA decisions within CMS-mandated timeframes as of October 2025 (Cohere Health survey). 78% of patients have abandoned treatment due to PA delays (AMA).
Staff burnout and FTE drain: Practices employ an average of 2.1 FTEs dedicated solely to PA management (MGMA 2025). 89% of physicians report PA contributes to burnout. These are clinically trained staff spending their time on administrative tasks instead of patient care.
Zero patient visibility: Patients have no way to check their PA status. As one physician noted: “You have more visibility into your pizza order than a life-saving medication going through prior authorization.”
CMS Programs Forcing the Fix: 5 Mandates You Cannot Ignore
2026 marks the most consequential year for PA reform in US healthcare. Five concurrent CMS programs and federal initiatives are creating both compliance obligations and strategic opportunities for every healthcare organization.
CMS-0057-F (Interoperability & Prior Authorization Final Rule): The master regulatory framework. Operational provisions took effect January 1, 2026 — payers must now respond to urgent PA requests within 72 hours and standard requests within 7 days, provide specific denial reasons, and begin collecting PA metrics. By January 1, 2027, payers must implement FHIR-based Prior Authorization APIs, Patient Access APIs, Provider Access APIs, and Payer-to-Payer APIs. CMS estimates $15 billion in savings over 10 years.
MIPS Promoting Interoperability — Electronic PA Measure: Starting CY 2027, MIPS-eligible clinicians must attest to submitting at least one PA electronically via a FHIR-based Prior Authorization API. Reporting “no” results in a zero score for the entire Promoting Interoperability category — a significant financial penalty affecting CY 2029 MIPS payments. Eligible hospitals and CAHs face the same requirement under the Medicare Promoting Interoperability Program.
WISeR Model (Wasteful and Inappropriate Service Reduction): Launched January 2026, this 6-year CMS Innovation Center pilot introduces AI-driven PA into Original Medicare for the first time — in 6 states (NJ, OH, OK, TX, AZ, WA) affecting 6.4 million beneficiaries. Six technology companies (Cohere Health, Genzeon, Humata Health, Innovaccer, Virtix Health, Zyter) use AI and ML for medical necessity review with 72-hour decision timelines. A gold-card exemption program launches mid-2026.
Improving Seniors’ Timely Access to Care Act: Bipartisan legislation re-introduced in the 119th Congress (S.1816, May 2025) with 50+ Senate cosponsors. Would mandate electronic PA standards for Medicare Advantage, real-time decisions for routinely approved services, gold-card programs, transparency requirements, and a ban on fax and proprietary payer portals. The Act also requires reporting on how AI impacts patient access and health equity.
AHIP 53-Insurer Pledge: 53 major insurers — including UnitedHealthcare, Elevance, Aetna, Cigna, Kaiser Permanente, Humana, and multiple Blue plans — committed to reducing PA scope, honoring 90-day care continuity when patients switch plans, and achieving 80% real-time electronic PA approvals by 2027. AHIP’s first public progress report is expected Spring 2026.
Top 5 Companies Leading PA Automation in 2026
| Company | Company Key Innovation | Key Innovation Results |
| Cohere Health | AI clinical intelligence platform. Auto-approves 90% of PAs. Cohere Align™ personalizes PA by provider track record. $200M funded. | 63% fewer denials, 15% lower medical expenses (Geisinger). 55% less provider submission time. 12M+ PAs annually. CMS WISeR participant (TX). |
| Waystar (WAY) | Auth Accelerate — end-to-end PA automation. AltitudeAI™ with generative AI for appeals. Best in KLAS for Patient Access. | 70% reduction in submission time. 85% auto-approval rate. 75% faster payer decisions (4+ days to <1 day). 30K clients. |
| Optum (UHG) | Digital Auth Complete + InterQual Auth Accelerator (Feb 2026). Connects 250+ payer systems. Powered by Humata Health. | 45% fewer manual touches. 80% efficiency in document bundling. 96% first-pass approval rate. Largest clearinghouse for X12 278. |
| Innovaccer | Flow Auth — AI-powered end-to-end PA within Healthcare Intelligence Cloud. Strong EHR integration and compliance dashboards. | CMS WISeR participant (OH). Enterprise health system client base. Regulatory compliance dashboards for PA workflow. |
| CoverMyMeds (McKesson) | Largest pharmacy ePA network. Connected to 75% of EHRs, 950K+ providers. ePA starts therapy 13 days sooner. | 3x faster than phone/fax. Millions of ePA requests processed. Transitioning to Surescripts for some payers. |
ROI That Justifies the Investment
The return on PA automation is not theoretical — it is documented across industry benchmarks and live deployments. CAQH projects $437–$494 million in annual industry savings by converting remaining manual PA to fully electronic transactions. Per-provider savings range from $74,000 to $145,000 per full-time authorization specialist through task automation. Patient care delays drop from 2–14 days to 0–2 days for electronically adjudicated authorizations.
At Geisinger Health Plan, deploying Cohere Health’s platform produced a 63% reduction in PA denials and a 15% reduction in total medical expenses — a direct bottom-line impact that extends far beyond administrative savings. Waystar’s Auth Accelerate clients report 85% auto-approval rates, compressing submission times by 70% and payer wait times from over 4 days to under 1 day. The 2025 CAQH Index confirmed that US healthcare avoided $258 billion in administrative costs through electronic transactions in 2024, with PA remaining one of the highest-opportunity areas for further automation.
The Window Is Closing: Strategic Recommendations
Prior authorization is at an inflection point. Federal mandates, AI-driven automation, and industry commitments are converging to transform PA from a manual, fax-era bottleneck into a real-time, API-driven, clinically intelligent workflow. Organizations that treat 2026 as a compliance checkbox will struggle. Those that invest now in FHIR-based infrastructure, AI-powered clinical review, and automated documentation assembly will gain a structural advantage — faster revenue cycles, lower denial rates, reduced staff burnout, and better patient outcomes.
The three pillars — interoperability (FHIR APIs and Da Vinci IGs), automation (RPA, DTR, rules-based engines), and AI (NLP, ML prediction, clinical nudges) — must be deployed together to address the full chain of PA failures. No single technology solves the problem alone. The organizations that thrive in 2027 will be those that recognized 2026 as the preparation year and acted accordingly.
